

Overall description
This research aims to develop and test a new method of promoting mental health among young people at upper secondary schools. The compensatory mission of schools makes them a key and important arena for various health-promoting activities and for the mental health of young people. Likewise, the mental health of young people is important for schools and for society, as young people who have mental well-being find it easier to learn things and are thus in a better position to achieve in school.

Background
One current problem is that there are no methods to promote the mental well-being of students in Swedish upper secondary school, with a proven effect [1]. There are methods to prevent mental problems (e.g. stress), mental illnesses (e.g. depression) and attempted suicide [2,3,4,5,6]. However, their principal point of departure is not mental health – as something positive – but rather the symptoms, condition or suffering that they are designed to prevent. One feature that these methods have in common is their focus on (socioemotional) problems instead of well-being and solutions. Some are also governed by psychological theories and models from a therapeutic tradition adapted to a specific target group rather than to all students. Swedish research has shown that problems may then arise when using them as universal initiatives [7].
When we adopt a problem or mental illness perspective to improve mental well-being, we diminish what mental well-being actually is
[8]. On the other hand, when we work on mental well-being and solutions we promote healthy functioning. The interventions need to be designed with a clear focus on factors that build up and strengthen well-being. The objective of Solution-focused Intervention for Mental health (SIM) is to produce such an initiative adapted for young people in their late teens. SIM is intended for all students and has been designed as a school-based multicomponent positive psychology intervention [2].
Theoretical points of departure
SIM is founded on two theoretical parts. One involves mental health, i.e. the target of the initiative itself – what is being promoted. The theoretical basis of this is the definition produced by the World Health Organisation, as …
”… a state of mental well-being in which an individual realises his or her own abilities, can cope with the normal stresses of life, can work productively and is able to make a contribution to his or her community”. [9]
This clearly shows that mental health is essentially a positive state that encompasses both hedonic [10,11] and eudaimonic well-being [12,13,14], i.e. both emotions as well as psychological and social aspects of function. This point of departure has been used to both design the intervention itself, including its different topics (see the flow chart), and to follow it up and evaluate it in a way that is psychometrically satisfactory for the target group [15].
The second part deals with the method, i.e. what governs how the promotion will happen. In SIM, this is done using solution-focused coaching based on a solution-focused approach and techniques. The latter derives from solution-focused brief therapy [16], a discussion method adapted for shorter initiatives, which should be particularly appropriate in a school context where there is no scope for very broad initiatives [17]. What differentiates solution focus from other discussion methods and programmes is that solution focus is not governed by psychological theories of how people function and the underlying cause of their problems. Instead solution focus deals with how people construct and grasp reality and their actions via language [18]. Dialogue is key; communication creates experiences and affects behaviour; behaviour and meaning are interrelated.
One key assumption of solution focus is that an attempt to investigate problems does not always clearly comprise a step towards solving them [19]. It may be more helpful to focus on ‘solution’ stories instead. Problems are rarely static; there are always times when things are slightly better. By shifting the focus from problems and shortcomings to moments when things are functioning, and also focussing on the client’s resources, the client can start to take small steps to improve things [18]. In this way, the coach and client can co-construct solutions to progress towards the future they want. A supportive and key starting point for SIM is that we focus on growth. How, why and the function of the co-creating process in a solution focus and its impact on a general level is documented in a systematic summary by Franklin and colleagues [20]. However, there are currently no randomised controlled studies of solution focus as a method for promoting mental health in the school environment. A randomised study of solution focus among young people was recently published, but the outcome of this was to prevent mental problems [21], not principally to promote mental health.
Based on the above two theoretical perspectives, the SIM method was designed to
- include topics that reflect the theory of mental health and how it is measured and evaluated
- be governed by a solution-focused approach and techniques
- enable it to be implemented as far as possible within existing structures in a school environment
- enable it to be implemented by specially trained mentors in schools
- enable it to be implemented in groups
- not be too extensive, but at the same time be enough to be expected to have an impact on mental health.
Method development and preliminary findings
The development of SIM started during the autumn of 2018 together with various activities in preparation for the research, such as compilations of ethical applications, research plan, questionnaire instrument and interview guides. The first implementation study, including the training of mentors and testing of methods at three upper secondary schools in Västerås, was implemented during the Spring Semester of 2019.
Flow chart of the first feasibility study
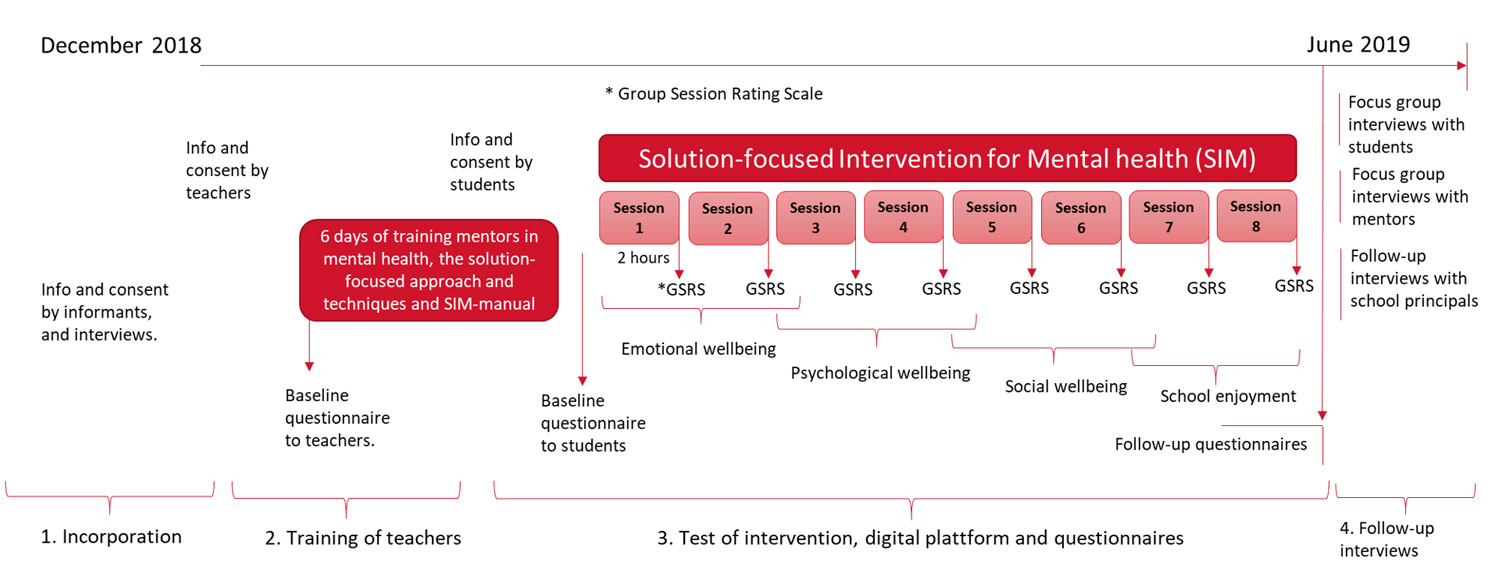
This study resulted in several important lessons being learnt, for example
- that the intervention should be held during the autumn to avoid clashes with, among other things, national examinations
- to liven up the manual and training material to make them more suitable for young people
- to include support films to introduce the topics of the intervention and working method
- to change the order of the intervention’s topics according to the level of abstraction
- to get backing for the study at an early stage – at least a year before the study starts – in order to incorporate SIM into the school curricula.
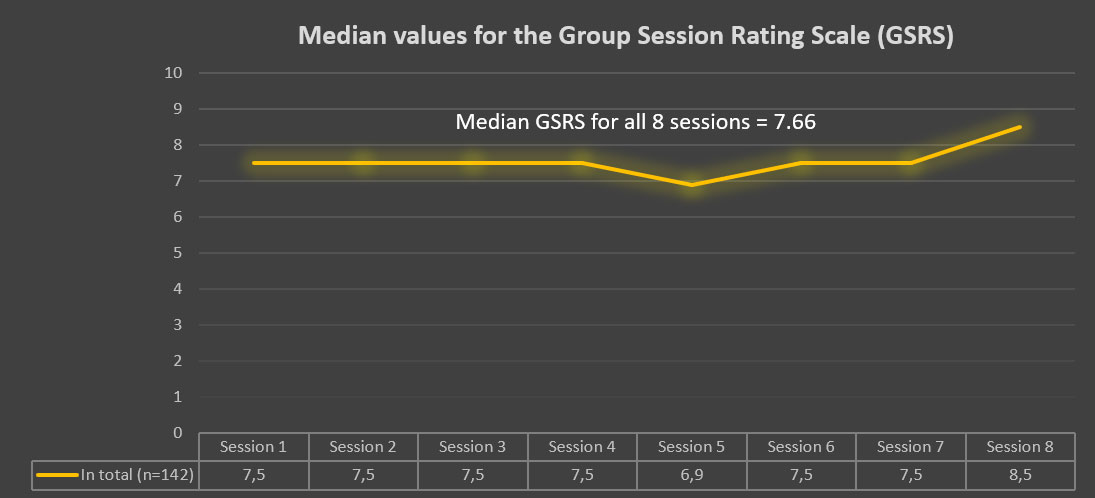
Another important finding, and possibly the most important, from the first sub-study comes from discussion ratings given at the end of each discussion session. These ratings involve the quality of the sessions (discussion alliance in group) and are based on Miller’s Group Session Rating Scale (GSRS). GSRS has four components relating to: form, content, how you feel that you were listened to and also the session as a whole [22]. The findings from the first sub-study show that when the median values for GSRS ratings of sessions are seven or above (on a scale of 0 to 10), this suggests that the method will have a statistically significant positive effect on mental well-being; see figure below. This is based on paired tests, where the level of mental well-being after the initiative is compared with the level before the initiative. Another finding, which is also important, is linked to student participation, where students need to attend five of the eight sessions for a statistically significant improvement in mental health to be seen. The latter underlines the importance of backing from an early stage and for SIM to be incorporated in the school curricula.
Revision and improvement of the method
In light of the above findings, work to review and improve the method has been underway since the autumn of 2019. This work includes revising both the content of sessions and the method manual and working material for participants. There has also been a major investment in a digital platform adapted for the SIM method, where all of the material was digitalised, and seven short films have also been produced to introduce the various topics for SIM. The digital platform offers, among other things, real-time feedback on the quality of discussions, which teachers can use as a basis for discussions on how sessions could be improved or to maintain good quality.

The second phase of the method development, was carried out in additional schools during the autumn of 2021 and will continue during spring 2023.
SIM now comprises nine extended sessions, each of two hours, at approximately weekly intervals. The sessions are coaching solution-focused meetings, where participants can work as a full group of 10 to 15 students, as a resource team of three to five students and also individually. Further information about the method can be found under the ‘The SIM method’ tab.
After the method with its associated procedures has been tested and verified in the feasibility phase, a proper evaluation of the promotional effect on mental well-being will be performed in a randomized controlled trial planned for the spring of 2025.
References
The links below will open in a new tab.
- SBU. Universella program i skolan för att främja psykisk hälsa bland unga 2016 [Available from:
Universella program i skolan för att främja psykisk hälsa bland unga 2016 – SBU (pdf) - Tejada-Gallardo C, Blasco-Belled A, Torrelles-Nadal C, Alsinet C. Effects of School-based Multicomponent Positive Psychology Interventions on Well-being and Distress in Adolescents: A Systematic Review and Meta-analysis. Journal of Youth and Adolescence. 2020, 49(10):1943-1960.
- Garmy P, Clausson E, Berg A, Steen Carlsson K, Jakobsson U. Evaluation of a school-based cognitive–behavioural depression prevention program. Scandinavian Journal of Public Health, 2019; 47: 182–189
- Franklin C, Kim J, Beretvas T, Zhang A, Guz S, Park S, Montgomery K, Chung S, Maynard B. The Effectiveness of Psychosocial Interventions Delivered by Teachers in Schools: A Systematic Review and Meta-Analysis. Clinical Child and Family Psychology Review. 2017; DOI 10.1007/s10567-017-0235-4.
- Wasserman D, Hoven CW, Wasserman C, Wall M, Eisenberg R, Hadlaczky G, Kelleher I, Sarchiapone M, Apter A, Balazs J, Bobes J, Brunner R, Corcoran P, Cosman D, Guillemin F, Haring C, Iosue M, Kaess M, Kahn JP, Keeley H, Musa GJ, Nemes B, Postuvan V, Saiz P, Reiter-Theil S, Varnik A, Varnik P, Carli V. School-based suicide prevention programmes: the SEYLE cluster-randomised, controlled trial. Lancet, 2015;385(9977):1536-44.
- Livheim F, Hayes L, Ghaderi A, Magnusdottir T, Högfeldt A, Rowse J, Turner S, Hayes S, Tengström A. The Effectiveness of Acceptance and Commitment Therapy for Adolescent Mental Health: Swedish and Australian Pilot Outcomes. Journal of Child and Family Studies. 2014; DOI 10.1007/s10826-014-9912-9.
- Kvist Lindholm S. The Paradoxes of Socio-Emotional Programmes in School Young people’s perspectives and public health discourses. Linköping Studies in Arts and Science No. 664. Department of Thematic Studies – Child Studies Linköping 2015.
- VanderWeele T, Chen Y, Long K, Kim E, Trudel-Fitzgerald C, Kubzansky L. Positive epidemiology? Epidemiology. 2020; 31(2), 189–193.
- World Health Organization (2013). Mental health action plan 2013–2020 (pdf) Accessed 31 October 2020.
- Diener E. Subjective well-being. Psychological Bulletin. 1984;95(3):542-75.
- Kahneman D. Objective happiness. In: Kahneman D, Diener E, Schartz N, editors. Well-being: The foundations of hedonic psychology. New York: Russell Sage Foundation; 1999. p. 3-25.
- Huppert FA. Psychological Well-being: Evidence Regarding its Causes and Consequences. Appl Psychol. 2009;1(2):137-64.
- Ryff CD. Happiness is everything, or is It – explorations on the meaning of psychological well-being. Journal of Personality and Social Psychology. 1989;57(6):1069-81.
- Keyes CL. Mental illness and/or mental health? Investigating axioms of the complete state model of health. J Consult Clin Psychol. 2005;73(3):539-48.
- Söderqvist F, Larm P. Psychometric evaluation of the mental health continuum – short form in Swedish adolescents. Current Psychology. 2021;
Psychometric evaluation of the mental health continuum – short form in Swedish adolescent - de Shazer S, Dolan Y, Korman H, Trepper T, McCollum E, Berg IK. More than miracles: The state of the art of solution-focused brief therapy. New York: Haworth Press; 2007.
- Perkins R. The effectiveness of single session therapy in child and adolescent mental health. Part 2: An 18-month follow-up study. Psychology and Psychotherapy: Theory Research and Practice. 2008;81(2):143-56.
- de Shazer S. Words were originally magic. New York Norton; 1994.
- de Shazer S. Clues: Investigating solutions in brief therapy New York, US: W W Norton & Co.; 1988.
- Franklin C, Zhang A, Froerer A, Johnson S. Solution-focused brief therapy: a systematic review and meta-summary of process research. Journal of Marital and Family Therapy. 2016; Doi: 10.1111/jmft.12193.
- Wallace L, Hang Hai A, Franklin C. An Evaluation of Working on What Works (WOWW): A Solution‐Focused Intervention for Schools. Journal of Marital and Family Therapy. 2020; 46(4):687-700.
- Quirk K, Miller S, Duncan B, Owen J. Group Session Rating Scale: Preliminary psychometrics in substance abuse group interventions. Counselling and Psychotherapy Research. 2012;1-7.